For my externship in our MSBS program, I have chosen to work in the Pathology department at CU Anschutz in Aurora, Colorado. As a part of the experience, I was invited to observe and participate in an autopsy this past Tuesday, November 21, 2021.
The autopsy was led by Dr. Bala, and was assisted by a second-year resident, a first-year resident, a third-year medical student, and me. The patient was a 91-year old female who had passed away two days prior from complications arising from lung cancer. The patient and her family had opted to donate her body to the hospital to be used for teaching. The third-year resident started the autopsy by identifying the patient and any markings (tattoos, scars, hair color, eye color, etc) and reviewing her medical history and cause of death. Dr. Bala then took over and opened the patient.
The evisceration was performed swiftly, and it was immediately apparent that the patient had suffered at least a partial bowel obstruction, as there was odorous, brownish-green fluid in the abdomen. The pathologist separated and removed the small and large intestines, excising them at the level of the duodenum proximally and the rectum distally. The intestines were then washed, placed in a basin, and set aside. After this was completed, the abdominal fluid was removed and measured (about 500 mL). The chest plate was then removed using a bone saw, and was placed by the patient’s head on the gurney. From there, the pathologist excised the remaining visceral organs in one piece, from the trachea to the remaining portion of the duodenum, and placed them on a wooden block by the sink. The remainder of the autopsy focused on separating and examining each visceral organ. Dr. Bala would remove the organ and pass it to the second-year resident Askia, who would weigh it and grossly examine it before passing it to third-year resident Jessie, who would dissect the organ and remove samples to go to the Pathology department for processing and eventual microscopic examination. I was invited to be involved in the process, and was able to feel and grossly examine every organ. Some items of note from my examination:
Patient had multiple adhesions and enlarged lymph nodes in the thorax, due to probable radiation therapy for her lung cancer and history of breast cancer.
Missing breast tissue on the right due to history of unilateral mastectomy for breast cancer (left breast tissue was removed and sent to pathology for examination).
Aorta was highly calcified; felt “crunchy” when touched. Same thing was felt with the right and left atrioventricular coronary arteries.
Right atrium was very dilated, about 2-3 times as large as normal, and the tricuspid valve was mildly dilated, indicating the high likelihood of pulmonary hypertension.
Patient had mild scoliosis of the thoracic spine; per the pathologist this is very common in elderly people. The vertebrae themselves were osteoporotic.
Gallbladder was very dilated and contained a large stone; stone was calcified, black, and the same size and shape as a kidney bean.
The pancreas looks very similar to adipose tissue; it is lobular and yellow. The pancreas is much more solid and formed than adipose tissue.
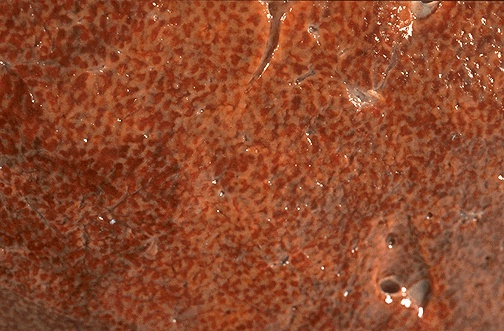
The liver had a “nutmeg” appearance, which is pathologically significant in that it indicates chronic liver congestion secondary to right-sided heart failure.
Patient had no organs of reproduction and had her left second toe amputated due to peripheral venous insufficiency.
Patient had pitting edema in the right arm due to a buildup of extracellular fluid; this was not present on the left side. Dr. Bala explained that this was due to the lack of lymph nodes and vessels on the right side, which were likely removed during the right-sided mastectomy for the patient’s breast cancer.
I was not able to observe the lungs, but was told that they were highly scarred due to lung cancer treatments.
The brain was not extracted for the autopsy. The brain is only extracted if there was neurological pathology, as brains have to fix in solution for two weeks before they can be processed. Additionally, brain extraction is not done as frequently due to family’s wishes for funeral proceedings.
Figure 1: Cut surface of the liver showing “nutmeg” appearance
The autopsy experience was highly educational, but very jarring and left me feeling many emotions. The whole procedure felt cold and rough, without the normal care and empathy that we associate with patient care.
Autopsies are still performed routinely (CU Anschutz performs around 100 autopsies every year), but they are being regarded as only marginally useful in modern medicine. However, an article on the importance of autopsies posits that, “that the autopsy remains an important procedure with substantial, if largely underused, potential to advance medical knowledge and improve clinical practice,” (Burton & Underwood, 2007). This experience has certainly worked to expand my own medical knowledge, and I am grateful to the deceased for offering me this opportunity to learn.
References
Burton, MEd, J. L., & Underwood, MD, S. J. (2007, April 28). Clinical, educational, and epidemiological value of autopsy. The Lancet, 369(9571), 1471-1480. 10.1016/S0140-6736(07)60376-6
This is a great post, Jen! I found it fascinating the aorta and coronary arteries were crunchy when performing the autopsy. After some further research, I found that aortic valve calcification narrows the heart valve reducing blood flow and can lead to heart failure (Lopez-Jimenez, 2021). A patient with cancer and aortic stenosis is difficult to treat due to the high risk the patient faces recovering from the most effective treatment, valve replacement (Kornowski, Landes, 2018).
ReplyDeleteReferences:
Kornowski, R., & Landes, U. (2018, April 20). The double jeopardy of aortic stenosis in cancer patients . Academic.oup.com. Retrieved November 29, 2021, from https://academic.oup.com/ehjqcco/article/4/3/150/4979550.
Lopez-Jimenez, F. (2021, February 19). Aortic calcification: an early sign of heart valve problems?Mayo Clinic. Retrieved November 29, 2021, from https://www.mayoclinic.org/diseases-conditions/aortic-stenosis/expert-answers/aortic-valve-calcification/faq-20058525.