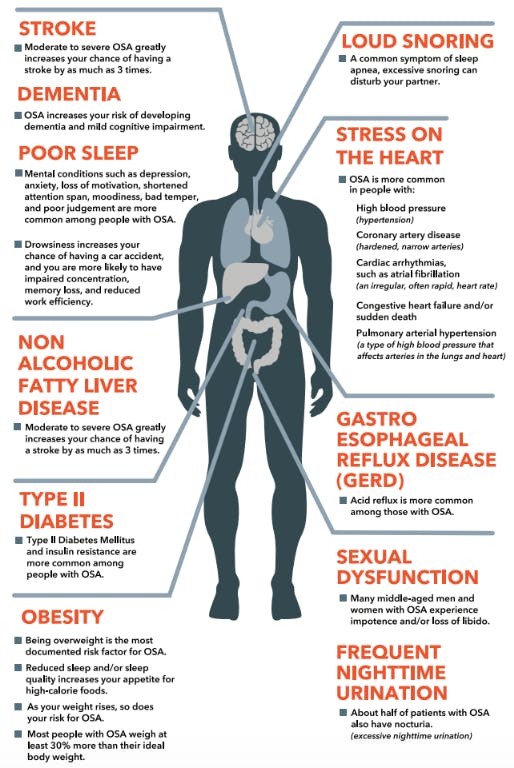
Obstructive sleep apnea (OSA) is one of the most common sleep disorders in North America, affecting approximately 15-30% of men and 10-15% of women (Kline, 2021). Obstructive sleep apnea is a condition characterized by the cessation of breathing during sleep; these cessations are known as apneas. OSA occurs when the airway collapses or is otherwise impeded (most commonly by the tongue falling back into the throat), cutting off air flow. The most common symptoms of OSA include: daytime sleepiness, loud snoring, choking, or gasping during sleep, and morning headaches.
Common risk factors of sleep apnea are obesity, craniofacial and upper airway abnormalities, older age, and being male (Kline, 2021). The severity of sleep apnea is measured using the Apnea Hypopnea Index (AHI), which is calculated by taking the sum of all the hypopneas and apneas and dividing them by the total hours of sleep (Schulman, 2020). Diagnostic criteria for OSA in adults is an AHI of 15, or greater than 5 with appropriate signs, symptoms, and comorbidities (Schulman, 2020).
Treatment of sleep apnea initially centers around two approaches: behavior modifications and continuous positive airway pressure (CPAP) therapy (Krieger & Malhotra, 2021). CPAP is typically considered to be the golden treatment for sleep apnea (Krieger & Malhotra, 2021). Other methods, including oral devices and surgical procedures, have varying levels of success (Krieger & Malhotra, 2021). However, a new treatment method has shown to be very promising for those sleep apnea patients who fail or do not tolerate CPAP: a hypoglossal nerve stimulator. At this time, Inspire is the only FDA-approved hypoglossal nerve stimulator in North America (Inspire Sleep Apnea Innovation, n.d.).
The Inspire implant is a small, battery-operated stimulator that is surgically implanted in a “pocket” in the patient’s chest, usually on the right side. The stimulator is smaller than a credit card and can be left in place for more than 10 years. A sensor, running from the stimulator, is wrapped around cranial nerve XII, the hypoglossal (“below tongue”) nerve; another is fed through the ribs to be near the diaphragm. The patient uses a small remote, about the size of a computer mouse, to turn the stimulator on at bedtime every night. After an electrical “pulse” that indicates the Inspire device is turned on and active, the device is on a delay to allow the user to fall asleep. Once asleep, the Inspire device stimulates the hypoglossal nerve and helps to maintain “tone” in the tongue, keeping it from falling into the back of the throat and obstructing the airway. The Inspire settings are customizable, from the length of the delays when falling asleep and while the device is paused, to the strength of the electrical impulses.

A study performed in 2014 on patients with hypoglossal nerve stimulators showed “significant improvement in the primary outcomes, including reduction in the frequency of respiratory events (29.3 events per hour at baseline to 9.0 events per hour at 12 months) and the oxygen desaturation index score (the number of times per hour of sleep that the blood oxygen level dropped by ≥4 percentage points from baseline; 25.4 to 7.4 events per hour)” (Malhotra, 2014). Additionally, even though hypoglossal nerve stimulators such as Inspire require surgical implantation, serious adverse effects are uncommon, only appearing in <2% of patients, and side effects are well tolerated (Malhotra, 2014).
I have OSA due to an anatomical abnormality called airway stenosis, in which my airway is narrowed. Added to that, I have a tongue that has a high rise in the back of my throat (characterized as a Mallampati class III). I have had sleep apnea for as long as I can remember, even when I was very thin. I had tried and failed CPAP and was suffering from many side effects related to OSA: daytime fatigue, morning headaches, irritability, depression, and GERD.

In the summer of 2019 I underwent surgery for the placement of the Inspire implant; due to my anatomy the surgery was described as difficult and took 5 hours instead of the usual 2.5 to 3, but everything worked out fine and I was discharged home the same day. After some moderate post-operative pain (mainly in my intercostal incision area), I returned to work. About 6 weeks later the Inspire device was turned on and I gradually increased the impulse strength until I was finally able to sleep all night and wake up feeling refreshed. To say this has been a life-changing experience is an understatement; my sleep has improved, and the majority of my OSA-related issues have resolved. I have minor side effects, including a perpetually swollen neck, but I feel this is a small price to pay for good sleep! Besides, the only thing better than one neck is two!
References
Inspire Sleep Apnea Innovation. (n.d.). Inspire Sleep. https://www.inspiresleep.com/
Kline, L. R. (2021, June 03). Clinical presentation and diagnosis of obstructive sleep apnea in adults. UpToDate. Retrieved October 03, 2021, from https://www.uptodate.com/contents/clinical-presentation-and-diagnosis-of-obstructive-sleep-apnea-in-adults?search=sleep%20apnea&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
Krieger, M. H., & Malhotra, A. (2021, February 23). Management of obstructive sleep apnea in adults. UpToDate. Retrieved October 03, 2021, from https://www.uptodate.com/contents/management-of-obstructive-sleep-apnea-in-adults?search=apnea%20hypopnea%20index&source=search_result&selectedTitle=4~65&usage_type=default&display_rank=4
Malhotra, A. (2014, January 9). Hypoglossal-Nerve Stimulation for Obstructive Sleep Apnea. The New England Journal of Medicine, 370(2), 170-171. 10.1056/NEJMe1314084
Schulman, D. (2020, March 19). Polysomnography in the evaluation of sleep-disordered breathing in adults. UpToDate. Retrieved October 03, 2021, from https://www.uptodate.com/contents/polysomnography-in-the-evaluation-of-sleep-disordered-breathing-in-adults?search=apnea%20hypopnea%20index§ionRank=1&usage_type=default&anchor=H86030600&source=machineLearning&selectedTitle=1~65&display_rank=1#H86030600
Jen! Thanks for sharing your experience! I have heard about these devices but I didn't know exactly how they worked or how they were implanted! I think it's so cool that this will hopefully be an easier option for people who can't tolerate the CPAP masks, I can't even tell you how many patients I've seen that can't stand them or won't even get tested for OSA in the first place because they know they won't wear the mask. Do all the sensors and the device need to be replaced after 10 years? Or is it just a generator/battery replacement? Just curious!
ReplyDeleteThanks Amber! From what my surgeon and Pulmonologist told me, its just the device itself that needs to be replaced at about 10 years; the sensors themselves do not need to be replaced unless something happens to them.
ReplyDeleteJen,
ReplyDeleteI love that you chose a topic that you had actual experience in because it gave insight to a patients opinion on the device. My dad tried and failed using the CPAP and is now trying out the DPAP. If that does not work out, I'm going to tell him to mention it to his doctor! I was looking into some articles about hypoglossal nerve stimulators and saw that it is still not widely used in pediatric settings just yet, but studies (the one I saw was specifically on children with trisomy 21) are proving have positive outcomes. I think this is an amazing alternative to the CPAP especially for children, who otherwise might not do so well sleeping with the mask it requires.
This is is the study: Hypoglossal Nerve Stimulator Placement for Pediatric Trisomy 21 Patients with Refractory Obstructive Sleep Apnea: A Case Series